Online
Archive
|
Online
Archive
|
| Issue 6 - June 1972 | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Everybody's Baby | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
 Although
the magnitude of the population problem is widely recognised, most
people
have come to accept it as a fact of life, and have largely ceased to
think about it. That is why constant reminders of the situation are
necessary and I hope this mention serves towards that end. Although
the magnitude of the population problem is widely recognised, most
people
have come to accept it as a fact of life, and have largely ceased to
think about it. That is why constant reminders of the situation are
necessary and I hope this mention serves towards that end.
There are many different aspects to this problem, such as the nature of growth of world population, the relationship of population growth and food supplies and the economic and social implications among others. But in this article, I will deal with contraception because when it comes to the crux of the matter, it is whether we are not going to limit our families which will dictate future population figures. 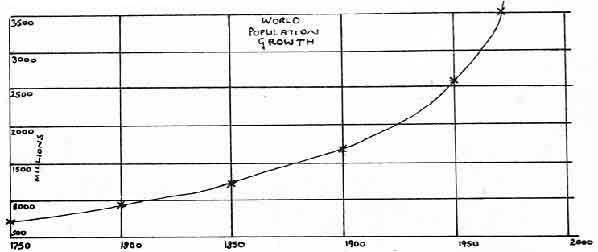
Take a look at the graph and ask yourself if we can afford to allow these figures to continue rising indefinitely. We all have a part to play in this matter and action must come now. We must not think of ourselves, but of future generations. When considering the actual methods of contraception available today, it is important to realise that no single method is yet suitable for every couple or situation. New methods are needed, especially for the male. An alternation of method between husband and wife would prevent or reduce long-term hazards of contraceptive methods to either one of them. The ideal contraceptive must be safe, acceptable, remote from intercourse, easy to use, cheap and readily available. Present day methods meet some of these requirements, but even the ideal contraceptive will require motivation on the part of the user. Set out in the table are the most widely used and readily available contraceptives. But as can be seen in the table, contraception is mostly left to the woman.
A contraceptive pill for men is possible, in the sense that researchers know what chemicals should be in one, but no-one has been given a clinical trial. The male contraceptive pill could work by stopping the development of the spermatozoa. But researchers are having difficulty in developing a suitable pill for men. They cannot seem to get the hormone content correct, plus all the synthetic male hormones that would work have the disadvantage of being poisonous and there is no chance of getting a vast supply of natural human masculine hormone. Another problem has been reported following a test in Australia. Men who took the pill went bald. It is a complicated problem. The tendency to baldness in men is inherited and therefore the genetic tendency may be activated by the male hormones that any male pill must contain. Also there is no financial incentive for manufacturing a male pill. The drug companies can see no good reason for working on the male pill because they realise that only half the population has to do anything about contraception. For every man who took the contraceptive pill, there would be one less woman taking hers. It looks as though the male contraceptive pill will stay at its present state, awaiting research and clinical trials. If you are in need of further information, contact your doctor, local public health department, or family planning clinic.
At this stage let us look at various family limitation programmes which have been set up in various parts of the world. India The arrival of intra-uterine devices (IUDs) on the scene in 1965 changed matters considerably. Because of the great clinical and administrative advantages of this method over sterilisation, an effective mass programme was now feasible. In the fourth five year plan, the budget was stepped up to 200,000 US dollars. Over the five years 1966-71, 20,000,000 IUD insertions were planned, 5,000,000 vasectomies, and it was hoped to have 10,000,000 effective users of traditional contraceptives. It is hoped by continuing these methods, to reduce the birth rate from about 40 per thousand total population to 25 per thousand by the year 1975, which will mean by then a reduction of about 9,000,000 births per year (birth in Britain is 16 per thousand total population). The impact of this programme on the national birth rate is as yet fairly small, but in certain areas cuts in the birth rate of between 10 and 20 per cent have been reported, and it has been officially estimated that about 1,200,000 births were prevented in 1967. Mainland China The Chinese press has advised late marriages for couples and suggested that families be limited to 2 or 3 children. In view of the effectiveness of the propaganda media in China, who can doubt that these recommendations will be followed? If they are followed successfully, this should prevent any catastrophic increase in numbers. Even so, it is still estimated that the population will exceed 1,000,000,000 by the end of the present century. Turkey Africa In the United Arab Republic, a nation of 30,000,000 people, a family programme has begun under the direction of the Supreme Council for Family Planning created in 1965 by the government. A large number of clinics offer advice and services, and large-scale manufacture of oral pills and IUDs is going ahead within the UAR, and these are distributed free of charge. In Ghana, independent surveys have already shown public attitudes which are consistent with the regulation of fertility, and it is thought that this is the attitude of other Central African countries, but in none of them has a family planning programme yet been implemented. Latin America Developed countries The Population Bomb, Paul Ehrlich, Pan Books, 30p Also Eco Publications are trying to make people more aware of the problem and other problems of the environment and they have published a book and various posters on the matter. Their address is 6 Cavendish Avenue, Cambridge. Ken The Family Planning Association In Newcastle and Sunderland special sessions are held for the unmarried who are seen by appointment. Telephone N/cle 39560 or Sunderland 69027 for appointment. For information about clinics see local telephone directories or telephone local branch administrators at Newcastle 27929 or Stockton 69902. Clinics on Teesside and in Darlington are now run by local health departments - for details telephone Middlesbro 43832 or Darlington 65218. The cost to an FPA private patient is £4.00 for the first year plus cost of supplies but many local authorities will pay for the advice.
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||